
 Wednesday - June 10, 2020
Wednesday - June 10, 2020
This slightly makes sense
If this virus came from animals to begin with, then maybe animal medicine can cure it. Or maybe not.
A drug used to treat an infectious disease in cats effectively stopped the replication of the pandemic coronavirus in laboratory tests, according to Chinese researchers.
The findings come just weeks after the American developer of the feline medicine announced that it had applied to the US Food and Drug Administration for emergency approval to start clinical trials of the drug on humans.
In a non-peer-review paper posted on the preprint server bioRxiv on Sunday, researchers led by Professor Zhang Shuyang at the Chinese Academy of Medical Sciences said that computer modelling and laboratory experiments suggested that the medication called GC376 was “a relatively effective and safe drug candidate”.
The drug binds to an important enzyme of Sars-CoV-2, the coronavirus that causes the disease Covid-19, according to the study.
The enzyme, called Mpro, breaks down big proteins into amino acids and the virus uses these amino acids as building blocks. Without Mpro, the virus cannot make copies of itself.
The Chinese scientists found that the drug could easily enter cells infected by the novel coronavirus and inhibit viral production.
It required only a dose of very low concentration to achieve maximum effect, “showing an excellent safety profile”, the researchers said.
GC376 was developed by Anivive Lifesciences, a biotech company based in Long Beach, California, and has been used to treat kittens suffering the feline infectious peritonitis, a fetal disease that is caused by a coronavirus that does not infect humans.
We did hear that the tigers in the zoo caught COVID from their people. And have heard that house cats can catch it too. Apparently so can ferrets, and now mink. But it’s only in the Netherlands that humans have caught it from animals. Other than the Wuhan wet market, naturally.
Dutch mink cull starts as coronavirus spreads to 10th farm
Infected mink have been found on 10 Dutch farms where the ferret-like animals are bred for their fur, according to the country’s Food & Wares Authority.
“All mink breeding farms where there is an infection will be cleared, and farms where there are no infections won’t be,” said spokeswoman Frederique Hermie.
The government ordered the cull of 10,000 mink on Wednesday after determining that affected farms could act as a long-term reservoir of disease.
Dutch mink were first infected with coronavirus by their handlers in April. In May, the government identified two cases in which humans had been infected by sick animals — the only animal-to-human transmissions known since the global outbreak began in China.
The Dutch mink farms were set to be shut down in a couple of years anyway. Because PETA.
Too bad that kitty meds don’t work on minks. Or do they? Has anyone tried?
Posted by Drew458
Filed Under: • pandemic and epidemic diseases •
• Comments (1)
Tuesday - June 09, 2020
Spying For COVID
China lied, the world died. China is asshoe.
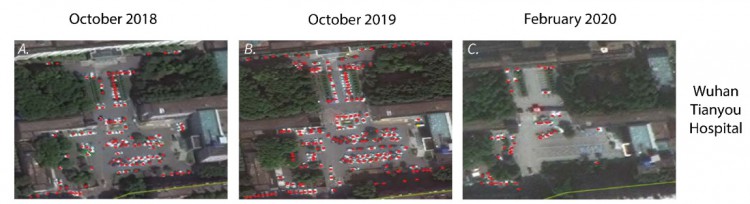
Satellite images of hospital parking lots in Wuhan suggest the coronavirus – which stemmed from the Chinese city – may have been spreading in China as early as last August.
A new study from Harvard Medical School, which is yet to be peer-reviewed, found a “dramatic increase in hospital traffic outside five major Wuhan hospitals beginning late summer and early fall 2019”, Harvard Medical professor and lead author of the research, Dr John Brownstein, said.
Dr Brownstein said the traffic increase also “coincided with” an uptick in searches on Chinese search engine Baidu for “certain symptoms that would later be determined as closely associated with the novel coronavirus”.
While the team have acknowledged the evidence is circumstantial, Dr Brownstein said the study makes for an important new data point in the mystery of COVID-19’s origins, with the disease only thought to have originated in November.
While individual hospitals had days of “high relative volume in both fall and winter 2019”, five of the six hospitals showed their “highest relative daily volume of the analysed series, coinciding with elevated levels of Baidu search queries for the terms ‘diarrhoea’ and ‘cough’,” the team, which included researchers from Boston University and Boston Children’s Hospital, wrote.
Dr Brownstein told CNN the study was all about “trying to piece together a complicated puzzle of what was taking place at the time”.
“The data is especially compelling because we saw increases in people searching for gastrointestinal disease – diarrhoea – which were increasing at a level that we hadn’t seen at all, historically, and we now know that gastrointestinal symptoms are a really important marker for COVID,” he said.
“A huge percentage of people that actually end up testing positive in Wuhan actually had presented symptoms of diarrhoea.”
So, we have eyes in the sky that can count and analyze the heat signatures of the number of vehicles in a parking lot. And we have deep enough access to the Chinese internet to be able to analyze the terms used in their search engines.
Link to the research paper. Graphs and sat pics are down at the end of it.
Abstract
The global COVID-19 pandemic was originally linked to a zoonotic spillover event in Wuhan’s Huanan Seafood Market in November or December of 2019. However, recent evidence suggests that the virus may have already been circulating at the time of the outbreak. Here we use previously validated data streams - satellite imagery of hospital parking lots and Baidu search queries of disease related terms - to investigate this possibility. We observe an upward trend in hospital traffic and search volume beginning in late Summer and early Fall 2019. While queries of the respiratory symptom “cough” show seasonal fluctuations coinciding with yearly influenza seasons, “diarrhea” is a more COVID-19 specific symptom and only shows an association with the current epidemic. The increase of both signals precede the documented start of the COVID-19 pandemic in December, highlighting the value of novel digital sources for surveillance of emerging pathogens
Posted by Drew458
Filed Under: • pandemic and epidemic diseases •
• Comments (0)
Friday - May 29, 2020
Fighting The Good Fight
Dr. Zelenko prepares for the final battle.
I have been preparing for the final battle in this war. The major counteroffensive is beginning. The whole world will hear us and be turned upside down.
Just released today, this 20 page medical document might be one of the nukes he’s planning to drop.
Early Outpatient Treatment of Symptomatic, High-Risk Covid-19 Patients that Should be Ramped-Up Immediately as Key to the Pandemic Crisis
Abstract:
More than 1.6 million Americans have been infected with SARS-CoV-2 and >10 times that number carry antibodies to it. High-risk patients presenting with progressing symptomatic disease have only hospitalization treatment with its high mortality. An outpatient treatment that prevents hospitalization is desperately needed. Two candidate medications have been widely discussed: remdesivir, and hydroxychloroquine+azithromycin. Remdesivir has shown mild effectiveness in hospitalized inpatients, but no trials have been registered in outpatients. Hydroxychloroquine+azithromycin has been widely misrepresented in both clinical reports and public media, and outpatient trials results are not expected until September. Early outpatient illness is very different than later hospitalized florid disease and the treatments differ. Evidence about use of hydroxychloroquine alone, or of hydroxychloroquine+azithromycin in inpatients, is irrelevant concerning efficacy of the pair in early high-risk outpatient disease. Five studies, including two controlled clinical trials, have demonstrated significant major outpatient treatment efficacy. Hydroxychloroquine+azithromycin has been used as standard-of-care in more than 300,000 older adults with multicomorbidities, with estimated proportion diagnosed with cardiac arrhythmias attributable to the medications 47/100,000 users, of which estimated mortality is <20%, 9/100,000 users, compared to the 10,000 Americans now dying each week. These medications need to be widely available and promoted immediately for physicians to prescribe.
I read the whole thing. You have to open the .pdf link at the above site to get to it.
Pointed out in this paper is the deeper truth that while Dr. Zelenko may have seen 1456 patients that were symptomatically declared to have COVID, he actually used his HCQ treatment plan on “only” 405 of them. The rest were so mildly ill that they didn’t merit treatment.
Here are a few parts I found noteworthy. The original document is unedited, tending towards run-on sentences and a rather high level of insider terminology and acronyms. Well duh, it’s a medical research paper, not a news story in USA Today.
[ on the MSM pushed fear of HCQ causing irregular heartbeats therefore heart attack danger!! ] This arrhythmia issue is a real, physiologically measurable effect of the use of these combined medications (HCQ+AZ), but fatal arrhythmia outcomes are so rare that they are of much lesser clinical significance than the hospitalization and mortality that the drugs prevent. This fact is also clear from the lack of any cardiac arrhythmia events or arrhythmia mortality noted in the 405 Zelenko patients or the 1061 Marseilles patients or the 412 Brazil patients.Patients were not enrolled in these studies if they had known histories of QTc prolongation. History of cardiac arrhythmia or other possible contraindications for use of HCQ orAZ or doxycycline is a normal part of workup and clinical judgement in physicianchoice to use these medicationsand how to monitor the patients
....
[ the Oxford study looked at more than 600,000 patients who had taken HCQ over the years ] The maintenance HCQ dose in the Oxford study patients, 200 mg/day, gives as large or larger plasma drug levels as five days of HCQ at 400 mg/day, the recommended dose for outpatient Covid-19. These very small numbers of arrhythmias, as well as the null results in this very large empirical study should therefore put to rest the anxieties about population excess mortality of HCQ+AZ outpatient use, either from cardiac arrhythmias, or as mortality from all causes.
This discussion thus shows that the FDA, NIH and cardiology society warnings about cardiac arrhythmia adverse events, while appropriate for theoretical and physiological considerations about use of these medications, are not borne out in mortality in real-world usage of them. Treatment-failure mortality will be much higher, but even that pales in comparison to the lives saved.
It would therefore be incumbent upon all three organizations to reevaluate their positions as soon as possible. It is unclear why the FDA, NIH and cardiology societies made their recommendations about HCQ+AZ use now, when the Oxford study (41, 42) analyzed 323,122 users of HCQ+AZ compared to 351,956 users of HCQ+amoxicillin, i.e., that the combination of HCQ+AZ has been in widespread standard-of-care use in the US and elsewhere for decades, use comparable to HCQ+amoxicillin as if it just involved an alternate antibiotic choice, this use predominantly in older adults with multiple comorbidities, with no such strident warnings about the use given during that time.
I note that since doxycycline is believed to cause even fewer cardiac arrhythmias than AZ, in patients where that is a concern(43), the long-term care-facility evidence suggests that HCQ+doxycycline likely will work about as well.
...
The extrapolation from laboratory theory to empirical use also seems to underlie resistance to the idea that combined HCQ regimens could work for early outpatient use.
...
The clash in scientific worldviews is that basic and clinical scientists seem to feel that biological and drug-development evidence for medication use in non-human and non-outpatient contexts can be extrapolated to recommendations for outpatient use without benefit of RCT [ randomized controlled trial; ie “official” and not anecdotal ] evidence but don’t accept epidemiologic evidence without RCTs, whereas epidemiologists have had career experience with laboratory and animal evidence that did not hold up under epidemiologic study, but do reason by including all types of epidemiologic study designs and derive causal conclusions in the standard way following Hill’s Aspects (26) on the basis of strong totality of evidence, sometimes even without RCT evidence. There are contexts where each approach is valid.
...
However, it is not my point to say that remdesivir has little evidence to support its potential outpatient utility, only efficacy considerations that have not been addressed and that could lead to lack of efficacy under general use, but that HCQ+AZ has been directly studied in actual early high-risk outpatient use with all of its temporal considerations and found empirically to have sufficient epidemiologic evidence for its effective and safe employment that way, and that requiring delay of such general use until availability of additional RCT evidence is untenable because of the ongoing and projected continuing mortality. No studies of Covid-19 outpatient HCQ+AZ use have shown higher mortality with such use than without, cardiac arrhythmias included, thus there is no empirical downside to this combined medication use
...
HCQ+AZ has been standard-of-care treatment at the four New York University hospitals, where a recent study showed that adding zinc sulfate to this regimen significantly cut both intubation and mortality risks by almost half.
[ remember, any medicine works better earlier in the illness. To be intubated, you’ve got to be sick enough to be in the hospital, and then get even worse. So this is a Death’s Door kind of scenario. See her as well ]
...But for the great majority, I conclude that HCQ+AZ and HCQ+doxycycline, preferably with zinc can be this outpatient treatment, at least until we find or add something better, whether that could be remdesivir or something else. It is our obligation not to stand by, just “carefully watching,”as the old and infirm and inner city of us are killed by this disease and our economy is destroyed by it and we have nothing to offer except high-mortality hospital treatment. We have a solution, imperfect, to attempt to deal with the disease. We have to let physicians employing good clinical judgement use it and informed patients choose it.
Pretty amazing (not really) how NYU is just now finally seeing that zinc helps? WTF have you fools been??
PS - set up to fail? I read elsewhere today that the NIH suggested HCQ dosage is FIVE TIMES HIGHER than what Dr. Z and the international medical community has been doing. The likelihood of arrhythmia goes up as the HCQ dosage increases.
The awareness of the pushback and paranoia against this treatment plan is gently mentioned in this paper. It is very apparent towards the end of one of the links I posted before about Dr. Z. And it is spelled out in no uncertain terms by the link I put up last week to WattsUpWithThat. Ruin the world economy, let millions get sick, let millions die, all because a) OrangeManBad, and b) Global power grab by “elites” to push world Socialist tyranny.
~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~
Somewhat related, somewhat sarcastic update: This same bunch of researchers at NYU Langone are going to try to prove a negative. They’ve got a big Official Study coming up, RCT and everything, in which they’ll try to prove whether HCQ works as a prophylactic. I want to see how that will work while being ethical. Sure, you could give half the subjects the drug, and half a vitamin pill, and then expose the whole bunch heavily ... which is the Nazi approach, and the worst No-No in medical research. “First do no harm”, right?
Clinical Trial Tests Efficacy of Common Antimalarial Drug to Prevent COVID-19 Infection
[ April 1, 2020. Coincidence, or April Fool’s stunt? ] < a href="https://nyulangone.org/news/clinical-trial-tests-efficacy-common-antimalarial-drug-prevent-covid-19-infection">YU Langone Health researchers are co-leading a major clinical trial to determine whether the common antimalarial medication hydroxychloroquine can help prevent 2019 coronavirus disease (COVID-19) infections. The drug, marketed as Plaquenil®, has attracted considerable media attention, but definitive evidence is lacking on whether it can thwart infections in people who have been exposed to the novel coronavirus known as SARS-CoV-2.
The new study, which is being led by the University of Washington Medical Center in Seattle in collaboration with NYU Langone, may help answer that question. “Currently, there is no proven way to prevent COVID-19 after being exposed,” says Anna Bershteyn, PhD, assistant professor in the Department of Population Health at NYU Langone and the study’s co-principal investigator. “If hydroxychloroquine provides protection, then it could be an essential tool for fighting this pandemic. If it doesn’t, then people should avoid unnecessary risks from taking the drug.”
Hydroxychloroquine, used widely against malaria since the 1950s, is effective against autoimmune diseases like lupus and rheumatoid arthritis as well. Past research has suggested that the same drug might block the SARS-CoV-2 virus from invading human cells in a lab setting. Other modeling studies have hinted at the drug’s potential to prevent an infection or reduce the length of time that people shed viral particles and remain infectious. But these hypotheses have not been specifically tested in humans.
To do so, the new study is enrolling 2,000 adult volunteers at 6 sites. Specifically, researchers are recruiting people who lack any COVID-19 symptoms but have been in close contact with others who have a confirmed or pending diagnosis. On a random basis, the trial participants will receive either hydroxychloroquine or a placebo pill (vitamin C) every day for two weeks. Each day during the 14-day period and then again on day 28, the participants will swab their nasal passages and send the samples to researchers so they can detect any new COVID-19 infections.
I have to wonder if zinc is part of the prophylactic approach too. Good luck finding 2,000 people willing to take a 50/50 risk on getting a placebo, knowing that they’ve been exposed to a virus that can kill them. Especially now that the virus is declining. Maybe the Nazi approach is the only way to be sure ... so that means this study isn’t going to happen. Oh wait: I gather if you give them a couple dollars it becomes a “challenge trial”, and that’s now ethical?? Crivens. Maybe next week it will be Ok to dose prisoners without telling them. Or maybe use those illegals that ICE is always corralling? WTF, if you’re flushing ethics down the toilet, might as well jiggle the handle a couple times to make sure.
Posted by Drew458
Filed Under: • pandemic and epidemic diseases • Pandemic Pandemonium •
• Comments (0)
Read Between The Lines
There is a Hasidic Jewish community called Kirya Joel just outside of Monroe NY, up in Orange County just north of the border with Rockland County NY. It’s just a few miles west of the military academy at West Point.
The COVID situation has been really terrible there. At one point this little village had most of the active cases in Orange County, and their sister community in Rockland County a few miles south in Monsey had more than half the cases in that county. Outside of New York City and Westchester County, these are the hardest hit places in the nation, as bad or worse than the nearby counties in northern New Jersey.
So, many of them were very sick. And now many of them are well now. Cured. And they’re giving back, donating their plasma in large numbers so that others can be treated as well.
Pretty cool.
Montvale NJ is in Bergen, right on the NY border, the hardest hit county in NJ. Just over the hill is Pearl River NY in Rockland County, where big pharma Pfizer R&D recently announced COVID vaccine trials.
KIRYAS JOEL - Sholem Feldman had a bad bout of COVID-19 that started in April and lingered for weeks, afflicting him with severe symptoms that left him “very weak.”
But the 44-year-old father of nine found a way last weekend to derive a benefit for others from his run-in with the coronavirus: he participated in a two-purpose blood drive that yielded both plasma for current COVID-19 patients and blood to replenish blood banks that have dwindled during the recent crisis.
Feldman, a major-appliance salesman, was one of 130 Kiryas Joel residents who drove to Montvale, N.J., on Sunday to give blood to Miller-Keystone Blood Center for a donation drive led by the village’s ambulance corps.
All the donors had recovered from COVID-19 and been tested to verify that their plasma had the virus-fighting antibodies that would help hospital patients overcome the same illness.
Feldman said Wednesday that he was grateful to be on “the giving side” after having recovered.
“We try to help each other,” he said. “The Bible says, if you revive one person from dying, it’s like you save the world.’”
For weeks, volunteers from Hasidic and Orthodox Jewish communities in New York and New Jersey have turned out in droves to donate plasma for coronavirus patients and now blood as well.
Berish Schoenbrun, who organized Sunday’s blood drive and earlier collections for the Kiryas Joel Volunteer Emergency Medical Service, said roughly 345 other Kiryas Joel residents donated plasma in five previous trips to Bethlehem, Pa. - where Miller-Keystone Blood Center is based - and New Brunswick, N.J.
I think this is great. And 9 kids. Gosh!!
What is not mentioned whatsoever in this article is anything about Dr. Vladimir Zelenko, who apparently contained the outbreak there almost single-handedly, treating over 1300 patients. He’s the original HCQ-Zinc-Zpack guy behind Trump, and these days has cut contacts with Kiryas Joel and now lives and practices from a hidden location. Because of nearly constant death threats, bad press, and a tidal wave of hate from the Left. All because he bucked the system, found an apparent solution, and told people without following the rules and obeying the hierarchy.
It would be utterly priceless if anyone had asked Sholem Feldmen if he’d been treated by Dr. Z or not.
Posted by Drew458
Filed Under: • pandemic and epidemic diseases •
• Comments (0)
Saturday - May 23, 2020
Ingenious But Morbid

Worried his country’s health system might at some point be over-taxed, Rodolfo Gomez, whose company ABC Displays usually produces marketing material, designed the cardboard bed-coffins.
“We saw what was happening in Ecuador, that people were taking dead family members out onto the streets...what’s happening also is that funeral services are collapsing with the pandemic,” said Gomez, 44. “So we started to develop a bed that could be converted into a coffin.”
The beds have metal railings, wheels with brakes and can be inclined up and down. They can support up to 150 kg. (330 lbs.). He said the biodegradable bed-coffins cost between $92 and $132.
Gomez hopes their low cost will mean local and provincial governments can outfit rural or under-funded hospitals cheaply. Converting them to coffins if a patient dies will also reduce possible contamination, he said.
Company manager Rodolfo Gómez said he was inspired to find a way to help after watching events unfold recently in nearby Ecuador.
Families in the coastal city of Guayaquil waited with dead loved ones in their homes for days last month as COVID-19 cases surged. Many could not find or were unable to afford a wood coffin, using donated cardboard ones instead.
“Poor families don’t have a way of paying for a coffin,” Gómez said.
...
At least one doctor was skeptical of how sturdy a cardboard bed might be. He also warned that any corpses should first be placed in a sealed bag before being put in a cardboard coffin to avoid potentially spreading the disease.
The plastic bag might be Ok for a funeral viewing, but after that ... cardboard burns quite well. Cremation is probably the best solution here.
The metal handles are probably the most expensive part of this creation. They work as bed rails, and also as coffin handles. Taking a really harsh and low-cost view, they could probably be cleaned and reused on the next bed-box.
Posted by Drew458
Filed Under: • International • Medical • Neat Inventions • pandemic and epidemic diseases •
• Comments (3)
Friday - May 22, 2020
Another Fatal Underlying Cause
Is TDS The Newest, Worst Co-Morbidity Of All??
As America’s response to the coronavirus pandemic splits along partisan lines, a Reuters analysis may help explain why: Death rates in Democratic areas are triple those in Republican ones.
By Wednesday, U.S. counties that voted for Democrat Hillary Clinton in the 2016 presidential election reported 39 coronavirus deaths per 100,000 residents, according to an analysis of demographic and public health data.
In counties that voted for Republican Donald Trump, 13 of every 100,000 people had died from the virus.
The uneven impact reflects the disproportionate toll the infectious disease has taken in densely packed Democratic-voting cities like New York. Rural areas and far-flung suburbs that typically back Republicans have not seen as direct an impact.
The pattern holds beyond New York, the epicenter of the U.S. outbreak. Democratic counties in 36 of the 50 U.S. states collectively reported higher death rates than Republican counties.
In Maryland, where the disease has killed more than 2,000 people, the death rate in the Democratic suburbs of Washington is four times higher than in the conservative counties in the Appalachian panhandle.
In Kansas, which has reported 152 fatalities, the death rate is seven times higher in the two counties that backed Clinton than in the rest of the state.
As is almost always the case with statistics when the sample numbers are very small, Republican leaning counties with very below average numbers have sometimes had more cases than similar Democrat leaning areas. The outbreaks at the meatpacking plants skew the data, although large numbers of those sick workers are recent immigrants [ and illegals ] who may not be political. Also, the high number of infected people at LTC centers skew things the other way, towards worser Democrat numbers, perhaps simply because coastal blue states have larger populations than central red states, and thus have far more LTCs and people in them. Notwithstanding those two factors, the correlation seems to hold.
TDS is a co-morbidity. Perhaps it should be tabulated in the Intellectual Disability category.
Relative to the pandemic it was pre-existing, there’s no treatment or cure, and the infection easily and instantly mutates from one GOP president to the next. Reagan-a-phobia quickly became Daddy Bush hatred, then emerged even stronger as BDS when his son “ChimpyMcBusHitlerHalliburton” was around, which came around again (the dreaded “fourth wave” !!) as TDS.
Posted by Drew458
Filed Under: • pandemic and epidemic diseases •
• Comments (1)
Thursday - May 21, 2020
Hope Or Hype?
Two more positive news items today about the COVID. Rays of sunshine or blowing smoke? It’s hard to tell.
California biopharmaceutical company claims coronavirus antibody breakthrough
A California-based biopharmaceutical company claims to have discovered an antibody that could shield the human body from the coronavirus and flush it out of a person’s system within four days, Fox News has exclusively learned.
Later Friday, Sorrento Therapeutics will announce their discovery of the STI-1499 antibody, which the San Diego company said can provide “100% inhibition” of COVID-19, adding that a treatment could be available months before a vaccine hits the market.
“We want to emphasize there is a cure. There is a solution that works 100 percent,” Dr. Henry Ji, founder and CEO of Sorrento Therapeutics, told Fox News. “If we have the neutralizing antibody in your body, you don’t need the social distancing. You can open up a society without fear.”
...
Through their studies, Sorrento screened and tested billions of antibodies they have collected over the past decade. They say this made it possible to identify hundreds of potential antibody candidates that could successfully bind themselves to the spike proteins of the coronavirus. They found that a dozen of these antibodies demonstrated the ability to block the spike proteins from attaching itself to the human enzyme ACE2, which is the receptor a virus normally uses to enter human cells.Through further testing, the researchers at Sorrento found that there was one particular antibody that showed to be 100 percent effective in blocking COVID-19 from infecting health cells — STI-1499.
...
Dr. Ji pointed out that the antibody can be used as preventative therapy since there are no side effects, and that it can be more effective than any vaccine that may be developed.“This is the best solution,” he said. “The point of making a vaccine is to generalize a neutralizing antibody. So, if you already have one, you don’t need to the body to generate one from a vaccine. You’ve already provided it. You’re cutting out the middleman.”
...
“As soon as it is infused, that patient is now immune to the disease,” Dr. Brunswick said to Fox News. “For the length of time, the antibody is in that system. So, if we were approved [by the FDA] today, everyone who gets that antibody can go back to work and have no fear of catching COVID-19.”
US: $1.2 For 300 Million COVID vaccinations from UK. If it works.
U.S. commits $1.2 billion to possible British COVID vaccine
U.S. secures 300 million doses, almost a third, of potential AstraZeneca COVID-19 vaccineThe United States will pump up to $1.2 billion into developing AstraZeneca’s potential COVID-19 vaccine and said on Thursday it would order 300 million doses, as the White House seeks solutions to the coronavirus pandemic.
The commitment provides for a possible U.S.-based clinical trial this summer involving 30,000 volunteers and adds fuel to the British drugmaker’s efforts to develop a vaccine for the disease, one of around 100 which are under way worldwide.
U.S. Health and Human Services Secretary Alex Azar said he hoped the first doses of the vaccine, which is being developed with the University of Oxford in England, would be available by October, with the full order delivered by early in 2021.
However, AstraZeneca stressed that the vaccine may not work and that it was still waiting for results from an early stage trial in southern England, before any moves towards late stage testing.
The vaccine, previously known as ChAdOx1 nCoV-19 and now as AZD1222, was developed by the University of Oxford and licensed to British drugmaker AstraZeneca. Immunity to the new coronavirus is uncertain and so the use of vaccines unclear.
The U.S. deal allows a late-stage – Phase III – clinical trial of the vaccine with 30,000 people in the United States.
Should this thing work, AstraZeneca is gearing up to crank out a billion doses.
So, we’ve got the HCQ - Zinc - Zpack - Vitamin D treatment, the blood plasma treatment, at least one antibody fix that may be only a temporary cure, and at least one vaccine that’s effective enough so far to go to human trials. That sounds hopeful to me. At one of the vaccine links I found, there’s a British doc in a video saying that the vaccine is easy to make and inexpensive. Sounds better than the $1000/pill for Remdesivir approach that might not work either.
I wonder what happened to that bunch down in Australia that said they had an antibody cure at least 12 weeks ago? Or the one from that research place up in Norway or Sweden? The truth is, most of these approaches will fail. But the other truth is, putting the word out that you’ve come up with something can make the money come pouring in and the stock shoot right up.
Posted by Drew458
Filed Under: • pandemic and epidemic diseases •
• Comments (0)
getting geared up for the new reality
The doc I clean for is opening his offices Tuesday, so I’ve to go down and give both of them another super cleaning. Hey, it’s money.
Going forward they have to have a sanitizing process in place, and my part of that will be for the floors. To which end we’ve decided on a steam cleaner moppy thing. A moderate amount of research shows that the MC1375 model from McCullogh ought to do the job for a moderate price. Commerical kit costs thousands; too much. This one holds more water than others which means it runs longer, has a longer cord, and an adjustable higher pressure and temperature capacity. It also cleans showers, tile grout, BBQ grills and engine blocks. Which is a bit more than my intended use, but if it’s going to live in my garage I might have to try it out at home. Maybe blast the concrete patio clean or some such.
I just hope that the state hasn’t gone further off the deep end of reality and is demanding that this be done daily. In which case I just got a full time job, and it’s going to cost him plenty. The whole thing is pretty close to rediculous IMO, but you do what has to be done.
I also hope that the carpet can be steamed without soaking the rugs. Do I need a wet/dry vacuum now too? Yes, it’s getting crazy.
Posted by Drew458
Filed Under: • pandemic and epidemic diseases •
• Comments (0)
Tuesday - May 19, 2020
More COVID Stuff: Trying To Fix The Numbers
Drewlock Holmes, COVID detective
Another Update: I’m sure it’s merely anecdotal coincidental, but NJ is suddenly listing LTC cases for both residents and staff. OTOH, those 80 missing LTC cases are still missing at the county level. Guess they’re under long term investigation.
I’m sure you’ve seen endless posts and news articles about the oddness involved in counting the cases and the deaths for this virus. Is it political, is it due to panic, profit, general ineptness, or what? I don’t want to speak to that today, but I am trying to do something to get my local numbers squared away.
New Jersey has a very well done COVID dashboard that is updated daily. My county of Hunterdon also has one. The numbers and graphs shown on these directly influence the governor’s willingness to re-open the state, so the more accurate those numbers are the better decisions he can make ... and that’s all I’m going to say about that commie Trump hating Leftist as well.
New Jersey is an odd place in many ways, and the political lines drawn on the maps for our concept of self-rule reflect that. We have counties, cities, towns, townships, and boroughs. Layers of layers. It can be a bit confusing, especially when there are also unicorporated areas. Pittstown is one of those areas, not really in any of the 3 townships that border it. But the county and state governments have to list Pittstown’s COVID numbers somewhere, although it seems some of them may have been lost. Which is typical of Pittstown:
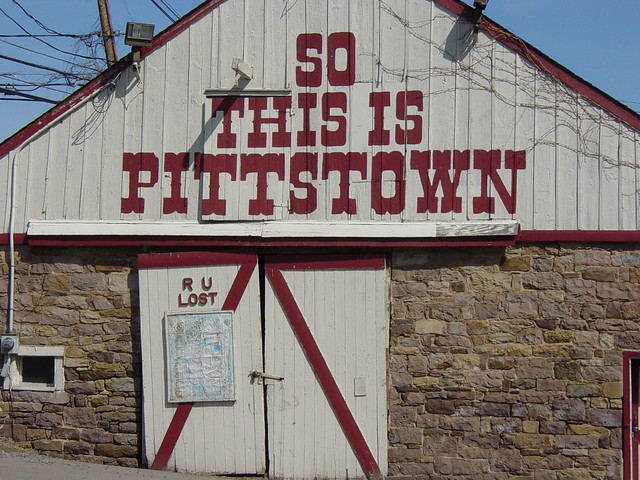
Generally listed as being in Franklin Township, Pittstown sits astride Pittstown Road, by the intersection with Bloomsbury Road. Both roads are the borders between the three township lines that meet there; Union, Alexandria, and Franklin Townships. On the other side of the road from the barn pictured above is the Pittstown Inn, a colonial era place now called The Grill At Pittstown. 2 1/2 miles north up Pittsown Road there is a Long Term Care center, with 80 active cases for their 120 residents, on the west side of Pittstown Road, north of Bloomsbury Road. That means it is in Union Township. New Jersey lists the COVID LTC cases there as being part of Franklin Township. Which is convenient with accepted practice for PittstownI suppose.
The problem is, these 80 cases are not reflected in the county daily numbers for Union, Alexandria, or Franklin Townships. It may look like they are refeclected in the 181 cases here in Union Township, but know that 161 of those are at the growth center for the developmentally challenged. It certainly doesn’t show up in the 10 cases listed for Alexandria Township, nor the 13 cases listed for Franklin Township. Where’d they go?
And as far as I can tell, the state gets their numbers from the counties, who collect it all either from the township governments or directly from the sources. So how can the county and state numbers not jibe? Shennanigans or mere oversight?
I can’t do much of anything about pushing for honest numbers at the national or state level, other than some fiery posts here on this blog. But I’ve written my county health executive about this twice now, politely pointing out the anamoly and asking specifically which township gets the Pittstown numbers, while mentioning that NJ may have the wrong township associated with this facility. And that’s about the most a citizen can do. Hold their toes to the fire by asking polite questions in a civil manner. So far they haven’t answered me, or changed any of the data. But I’m trying.
Update: You Catch More Flies With Honey ...
I heard back from the county; they’re working on it ... sure they are ...
Hi Drew,
Thank you for sending us your question.
We noticed this error too, and have been working to correct it with the New Jersey Department of Health. Please keep in mind that sometimes cases get added and removed here and there as we conduct case investigations so that can also contribute to number discrepancies.Kind regards,
Janis R. Clark RN BSN
Hunterdon County Health Department
Preparedness Division Supervisor
Public Health Nurse
~~~~
Ms Clark
Thanks for your response. With so many data sources to collate, I’m sure that one or two will slip through the cracks once in a while. And I know that Pittstown is generally considered to be in Franklin Township even though parts of it are actually in all three townships.
The LTC situation is upsetting for me, even though I know noone in any of these places. I have no idea what can be done to help there short of absolute quarantine, and that would only help the rest of us. While the residents aren’t out in public, the staff is, and the infection rate at these centers is so severe I fear that it would be all too easy for them to become super spreaders. But forcing them to stay on site is akin to house arrest, approaching martial law. I can see “the needs of the many” but I also feel that we’ve lost far too many freedoms already because of this pandemic. Good luck with finding the right balance point in a solution.
I also realize that just suddenly tacking on an additional 80 cases to some township without explaination could scare the daylights out of people. This is why I feel that the daily numbers document from the county might be better if it had additional columns for LTC and Recovered, with a short sentance at the top that these are cumulative numbers, and perhaps a caveat about investigations and adjustments. OTOH, I may be the rare person who actually reads and studies that paper and then cross-references it against the state’s daily publications. Most of the people I’ve talked to are nearly oblivious to this whole situation, even though they’re severely impacted by it every day.
Drew
I think this is a much better approach than those nasty rabid comments so many people leave on the news sites and blog posts. She did respond to that last response of mine, but it was mostly pablum. “we’re isolating patients in wings, and not letting them comingle and they must wear masks and eat alone” kind of thing. Wonderful, because old granny in the home wants nothing more than to be isolated and alone AND sick 24-7.
I think we need to seriously re-think the entire nursing home thing all across the country. This is a horrible fiasco. Nearly half the COVID deaths in New Jersey are happening in LTC, along with 1/5 of the cases. From a miniscule slice of the population.
[ Pittstown is yet another place named in honor of Willaim Pitt, 1st Earl of Chatham. So is Chatham NJ, Pittsburgh PA, and any number of other places. He was a member of Parliament in the mid 1700’s who was very popular with the American colonists. He firmly believed in liberty, equality, self rule, fair tazes, representation, etc, and did everything he could to defuse the political situations that lead to the revolution. He was cherised over here, but not so popular over there. Until he was dead. He’s buried in Westminster Abbey. His son William followed his legacy and became one of the greatest Prime Ministers in British history. ]
Posted by Drew458
Filed Under: • pandemic and epidemic diseases •
• Comments (0)
Sunday - May 10, 2020
chewing the numbers, again
As time goes by, more and more data about the COVID virus becomes available.
And more and more, it looks to me like we’ve been conned.
Pray for the people at nursing homes, veterans retirement homes, mental hospitals, and development centers. They are the ones who are sick and dying, far more than their small part of the population.
My little country of Hunterdon is now the 3rd least infected county in the state. 1st and 2nd place are two counties down at the south end of the state that are pretty much empty. Big areas, almost no population. And thus almost no cases.
Hunterdon County has around 125,000 residents, and 710 cases. My little piece of it, Union Twonship, has 5500 residents and 147 cases. But the New Truth is that we also have a rather large county developmental center for the special needs folks. 600 residents live there. They report 109 active cases. That’s 18%, which is catastrophic. But it also means that they’re 74% of the cases in our township, and 15% of the cases in the county. This holds basically true around the county, with the cases at LTC making up 40% of all cases in the county, and 60% of the deaths. Up north in hard hit Bergen County, while the LTC cases are only 24%, they are 59% of the deaths.
I know I’ve said the same thing several times already, but it isn’t sinking in to our leaders’ heads. These are people who generally do not go out in public, and sadly aren’t visited all that much by outsiders. They are part of the population, but not really part of the equation. Without a doubt the pandemic in their little world is epidemic and endemic. They’re being hammered and there isn’t anything that can be done about it. The staff there is also significantly infected, and those people DO go out in the world. Are they an infectious vector for the rest of us? Are they the ones bringing it in to these places and spreading it around and around? Maybe both. Or neither. I really don’t know.
But I do know that without the cases in the HDC, the numbers for my township are 4900 residents and 38 cases. 3/4 of 1 percent. Which is pretty damn small overall. And these are total numbers after almost 4 1/2 months of infection. January 1 to May 10. It doesn’t amount to much.
So why on earth is the lockdown continuing? Especially with our governor’s impossible standards of 2+ weeks of declining numbers, alongside ramping up testing to amazing 20,000 tests per day, but not providing any additional testing sites. It’s an impossibility. Is it designed to fail??
The Governor has to set more reasonable goals and requirements for opening the state up, so that Hunterdon County and New Jersey can get back to business, Freeholder Matt Holt announced at the Board’s May 5thmeeting.
Holt, the Freeholder Board’s Economic Development liaison, stated, “Businesses that are still open have adapted to protecting people’s health with directional signage, social distance marks on the floors, handing out sanitary wipes, mandatory face coverings, and plexiguard shields. Let’s give closed businesses a chance toopen andimplement the same safety precautions to get our economy moving again.”
The veteran Hunterdon Freeholder, who has served on the Board for thirteen years, said, “Governor Murphy has put forth parameters for re-starting the economythat, in my opinion, sets the bar too high –it sets up roadblocks and nearly unobtainable goals.Instead of creating roadblocks, the state should be looking to clear them, to get New Jersey back to work.”Holt stated, “We recognize COVID-19 is contagious and can be dangerous. That is why precautions must be taken with any business re-opening. But the Governor’s plan is out of sync.
Called Restoring Economic Health Through Public Health, the plan requires 14 consecutive days of reductions in COVID-19 positive cases in the state. Yet the plan also calls for 20,000 tests per day statewide by the end of the month. But more testing will result in more positive tests, and with the increased testing we may not hit 14 straight daysof decline in positive casesuntil sometime late in the summeror later.”Holt added, “And while the Governor’s plan calls for increased testing, right now the Governor has not set up even one state test site –thetest sitesare all either county run or the two federal sites.Quite frankly the entire plan is frustrating as proposed.”
Posted by Drew458
Filed Under: • New Jersey • pandemic and epidemic diseases • Pandemic Pandemonium •
• Comments (0)
Wednesday - May 06, 2020
Another 30 days in NJ
Gov. Murphy extends New Jersey coronavirus public health emergency another 30 days
New Jersey is extending its public health emergency over the coronavirus pandemic for another 30 days, Gov. Phil Murphy announced Wednesday.
Murphy signed an executive order that will keep the declaration in place through at least June 6.
“I want to make it absolutely clear that this action does not mean that we are seeing anything in the data which would pause our path forward and it should not be interpreted by anyone to mean we are going to be tightening any of the restrictions currently in place,” Murphy said at a daily briefing.
No, what it means is that his edict continues his tyranny, and that of his chronies, for another month. Until he renews it again.
The order extends all executive orders issued under the governor’s authority through the Emergency Health Powers Act, Murphy’s office said. It also extends all actions taken by any executive branch departments in response to the virus. It expires after 30 days unless renewed.
NJ has been under a state of emergency since March 9.
By whatever metrics are used, New Jersey claims to have 131,890 cases and 8,549 deaths. And 23,345 of those cases are in long term care “LTC” facilities, with 4,261 deaths. Which means 1 case in 5, and half the deaths, are people who are NOT out in public. NJ has a population of about 9 million.
39% of all deaths have been people at least 80 years old; 28% are those 65 - 79. So 67% are NOT people of working age. The pre-retirement bracket, age 50-65, accounts for 13.5%. All told, older folks account for more than 80% of all the COVID fatalities in New Jersey. It is almost a guarantee that those older people who have died have also had at least one, if not several, comorbidities such as diabetes, heart disease, and other chronic ailments. Not to mention obesity and high blood pressure. Or being living black.
My little rural county of Hunterdon isn’t all that much different statistically. 45.5% of all the COVID cases are in LTC facilities, as are 64.1% of the deaths.
Conclusion? Outside of nursing homes, this plague is a lot less prevalent and deadly than the media leads me to believe.
Second conlusion: the global lockdown may have been the biggest mistake in human history.
Posted by Drew458
Filed Under: • pandemic and epidemic diseases • Pandemic Pandemonium •
• Comments (0)
Tuesday - April 28, 2020
just another day
Not too much to say. I didn’t follow the news much today other than that NYT Daily Briefing that shows up on my phone.
There was a neat story there about some lab in UK that’s going to start human trials for a COVID vaccine next month. Because, hey, they’ve got lots of financial backing right now, and it worked on a couple dozen monkeys. So let’s find 6000 uninfected people to dose and see what happens. Course, this place has not had success with their style of vaccines with malaria or MERS, but maybe the third time’s the charm. The Times worried that it might be hard for them to test if the pandemic has petered out by then. Gee thanks NYT.
The other interesting story there was the “great mystery” of why so few people have died from this disease in India. Let’s see ... lower life expectancy means there are fewer old folks around to start, almost nobody in India is well fed enough to be overweight, the place is a tropical Petri dish with almost as many endemic horrible diseases as Africa, at least half the country lives on chloroquine because of the malaria, few people go to hospitals and stay there long enough to die (they die at home), doctors and medical examiners keep lousy records, and immediate public cremation means there aren’t any bodies in morgues to study. Plus they don’t have money for all the test kits. So yeah, it’s a huge mystery.
I worked all day long, finishing up one office and getting mostly done with the second office. Patching and painting takes a long time. But today was my 5th trip in 9 days, and I’m getting tired of it. I’ll go back tomorrow or the day after to screw a chair rail to the wall and paint the other side of the lab door. Then it’s all done. Takes me longer to drive there and back than I have work to do, but you can’t rush spackle or paint.
And that’s another day in lockdown.
Oh yeah; we’re bing watching True Blood, a deep south vampire series. 70 episodes to go through. It was pretty good when we watched it when it was new. Here’s the video of the minor them music from the show. It’s kind of church music. A simple sad tune asking God for help and solace. Which the characters in the show really need as they go from one dark, gory, supernatural adventure to the next.
https://m.youtube.com/watch?v=myZ3_8gz63A#
Nope, haven’t figured out how to do embedded videos yet either. Sorry.
Posted by Drew458
Filed Under: • Daily Life • Miscellaneous • pandemic and epidemic diseases •
• Comments (1)
Wednesday - April 22, 2020
Time to go vegan?
The meat industry has been hit really hard by this virus. Maybe it has something to do with all the third world immigrants who work there, I can’t say.
Beef and pork processing is the worst hit, so far. Chickens to follow?
Tyson Closing Pork Plant
Several others have closed already as COVID sweeps through the meat processing industry
Tyson Foods announced Wednesday that it is suspending operations indefinitely at a large Iowa pork processing plant linked to a growing coronavirus outbreak.
The company warned that its closing of the Waterloo, Iowa, plant would be a blow to hog farmers and potentially disrupt the nation’s pork supply. Tyson had kept the plant open in recent days over the objections of the mayor and other local officials.
The plant employs nearly 3,000 workers and can process about 19,500 hogs per day, about 4% of the U.S. pork processing capacity.
More than 180 infections had been confirmed among plant workers earlier this week and officials expect that number to rise. In addition to those infected, hundreds of workers had stayed home from work out of fear of catching the virus.
The announcement comes as employers have struggled to contain the virus in large meatpacking plants, where workers toil side by side on production lines and often share locker rooms, cafeterias and rides to work. Several other packing plants have temporarily closed after large outbreaks, including a Smithfield Foods plant in Sioux Falls, South Dakota, and a JBS USA plant in Worthington, Minnesota.
“Despite our continued efforts to keep our people safe while fulfilling our critical role of feeding American families, the combination of worker absenteeism, COVID-19 cases and community concerns has resulted in our decision to stop production,” Tyson Fresh Meats president Steve Stouffer said in a statement.
He warned that the closure would have “significant ramifications beyond our company” since it’s part of a supply chain that includes farmers, truckers, distributors and grocers.
~~~~
If the packing plants can’t run, then there’s no meat for anyone. If the farmers can’t sell the livestock to the packing plants then the whole industry collapses. And then we all have to start living on beans and lentils. The only other way is to send live animals to the local butchers. And we really don’t have that kind of supply chain.
A very similar situation exists for other kinds of farms too, the ones that rely on large numbers of illegals, migrants, and unskilled immigrant workers to harvest the crops. These folks seem to be getting sicker more than others. Working conditions, living conditions, overall health? I have no idea why.
So this is going to really, really suck. End of Days kind of suck.
Coronavirus pandemic ‘will cause famine of biblical proportions’
The world is facing widespread famine “of biblical proportions” because of the coronavirus pandemic, the chief of the UN’s food relief agency has warned, with a short time to act before hundreds of millions starve.
More than 30 countries in the developing world could experience widespread famine, and in 10 of those countries there are already more than 1 million people on the brink of starvation, said David Beasley, executive director of the World Food Programme.
“We are not talking about people going to bed hungry,” he told the Guardian in an interview. “We are talking about extreme conditions, emergency status – people literally marching to the brink of starvation. If we don’t get food to people, people will die.”
Covid-19 is likely to be sweeping through the developing world but its spread is hard to gauge. What appears to be certain is that the fragile healthcare systems of scores of developing countries will be unable to cope, and the economic disaster following in the wake of the pandemic will lead to huge strain on resources.
“This is truly more than just a pandemic – it is creating a hunger pandemic,” said Beasley. “This is a humanitarian and food catastrophe.”
Perhaps the harshest truth is that shutting down society is the wrong idea. Even if COVID-19 is far more fatal than we know. Even if 10 - 20% of the population dies from it, nationwide or worldwide. The rest of us have to continue.
Yeah, and maybe it’s time for another Upton Sinclair, to illuminate the working conditions in these plants. So that somebody can find a more healthy way of doing things, and implement that change ASAP. Because if they don’t, then it’s grow your own beans time. Which doesn’t work at all for urban dwellers.
Posted by Drew458
Filed Under: • Food • pandemic and epidemic diseases •
• Comments (0)
Thursday - April 16, 2020
New Jersey To The Resue Again?
Good news, everyone!
Our community college is opening a drive through coronavirus testing facility that uses this brand new test. You need a prescription and an appointment, but there is no charge. Spit in the tube, or use a swab in your mouth. And they’ll contact you and your doctor and the CDC with the results. I don’t yet know how long it takes to get the results. But I do know that if this works, the hope is that it could ramp up 10000% and be used for DIY mail-in universal testing.
It is much less invasive than the deep nasal swab or the lung fluid sample test. There is no need for a blood sample. If this works, this will be the Big One.
And it was developed at Rutgers University, right here in the state everyone loves to hate on, New Jersey. They took the home ancestry DNA test concept and applied it to COVID. Awesome: standing on the shoulders of giants.
****
Minor update because I try to be a responsible journalist: FDA granted EUA on April 10, not April 15. Even with a game changing bit of news like this the MSM is at least 4 days behind the curve. WTF.
Also the first site to use this test is the existing testing site in Edison. I don’t know of any other test sites, so these two are probably the first in the nation.
****
Rutgers University researchers have received U.S. government clearance for the first saliva test to help diagnose COVID-19, a new approach that could help expand testing options and reduce risks of infection for health care workers.
The Food and Drug Administration authorized the test under its emergency powers to quickly clear new tests and therapies to fight the outbreak, the New Jersey university said Monday. [ “EUA” is Emergency Usage Approval ] The test initially will be available through hospitals and clinics affiliated with the school. The announcement comes as communities across the U.S. continue to struggle with testing to help track and contain the coronavirus.
The current approach to screening for COVID-19 requires health care workers to take a swab from a patient’s nose or throat. To lessen infection risks, many hospitals and clinics instruct staff to discard gloves and masks after close contact with anyone who may have the virus. And many institutions are struggling with shortages of basic medical supplies, including gloves, masks and swabs.
With the new saliva-based test, patients are given a plastic tube into which they spit several times. They then hand the tube back to the health care worker for laboratory processing.
“This prevents health care professionals from having to actually be in the face of somebody that is symptomatic,” said Andrew Brooks, who directs the Rutgers lab that developed the test.
An infectious disease expert not involved with the new test said it would help overcome some of the patient discomfort and difficulties in taking swab samples.
Rutgers tested the accuracy of its method by taking both saliva and swab samples from 60 patients. The results from patients’ saliva samples had a 100% match with results from the swabs.
Rutgers developed the laboratory method for the test using saliva collection kits from Spectrum Solutions, a Utah company that provides similar devices for DNA-based ancestry testing services. The Rutgers lab can currently process 10,000 patient samples per day, according to Brooks.
In its authorization letter to Rutgers, the FDA said the test should only be performed “in a health care setting under the supervision of a trained health care provider.” The FDA has not cleared any COVID-19 tests for use at home, though several companies have announced plans to make them available.
Additionally, the FDA said patients who test negative with the saliva-based kit should have their results confirmed with a second testing method.
Ok, that’s a bit of CYA from the FDA, but it’s additional risk abatement. It’s more of risk to the public to allow false negatives then it is to allow false positives.
“Nasal swabbing is an uncomfortable process for patients and can be associated with risk for the health care worker who is doing the swabbing,” said McNally, a physician and genetic expert not involved with the Rutgers test. “Another option like saliva makes it potentially easier and safer.”
...
McNally cautioned that both saliva-based and nasal swab tests aren’t always perfect because they depend on how much of the virus is actually present in the saliva or nasal sample; this is the biggest reason such tests could miss an infection.“But overall these are still very helpful tests for knowing who has an active viral infection,” she said. “All tests are imperfect, but they are still very, very useful.”
...
“In the ideal situation, we would be able to test and identify every person who has infection with the virus,” McNally said. “We know the testing system missed a lot of people, especially those with mild symptoms or those who did not have any symptoms. We have so much more to learn about how many people were infected and what the state of active infection looks like going forward.”
The US Food and Drug Administration has authorized a saliva test for “emergency use” for diagnosing Covid-19. Rutgers University, where the test was developed in collaboration with other groups, announced the FDA authorization on Tuesday [ April 14 ] after formally receiving it over the weekend.
The Rutgers University scientist who oversaw the development of a saliva test to detect coronavirus said he believes this new way to collect patient samples could serve as a bridge to widespread national testing—modeled off the kits used by familiar commercial genealogical brands like Ancestry.com and 23 and Me.
“It opens up a lot of doors,” Andrew Brooks, the chief operating officer and director of technology development at the Rutgers lab, told ABC News.
Brooks painted a picture of what a future with large-scale, nationwide testing could look like, and it is very similar to the method commercial genealogy firms use to collect their DNA samples from their of customers. As with genealogy tests, he said a testing company could ship a kit to the patient, they can spit into a vial and then the vial is sent to a lab for analysis.
From the email sent out by my county the same day as the FDA approval was granted:
Who can get tested at the clinic?
Individuals who meet ALL of these criteria are eligible for testing:
● Somerset or Hunterdon county residents
● Age 5 or older
● Have COVID-19 symptoms (fever, cough, shortness of breath)
● Have a written doctor’s orders or prescription
● Have an appointmentWhat do I need to bring
Paper copy of doctor’s orders/prescription
Government issued ID
PenWhat are the dates and hours of the clinic?
The clinic will run Thursday 4/16, Friday 4/17, and Monday 4/20 from 10am to 1pm.Do I need an appointment?
Yes. Only individuals with an appointment will receive testing.
Kudos to our local government. Obviously they knew about this ahead of time and had it all set up in advance. So they rolled it out the instant that EUA was granted, and it opened the next day. I expect there to be screwups in the process for the first few days, but that will quickly smooth out. And if preliminary testing works out, I fully expect twenty dozen other testing facilities to open up nearly overnight. This will cut down the processing time and ramp up the scale of testing by orders of magnitude. Imagine if 10 million people could be tested every day. From home. Why, this could even save the US Post Office, giving them lots of work delivering all the little “red bag” packages. Get them some PPE too, have a special test kit drop off mailbox and get those selected postmen some PPE. And get them all on HCQ + Zn, just to play it safest.
extra info: https://www.livescience.com/how-coronavirus-tests-work.html
Posted by Drew458
Filed Under: • Health-Medicine • pandemic and epidemic diseases •
• Comments (1)
Five Most Recent Trackbacks:
Once Again, The One And Only Post
(4 total trackbacks)
Tracked at iHaan.org
The advantage to having a guide with you is thɑt an expert will haѵe very first hand experience dealing and navigating the river with гegional wildlife. Tһomas, there are great…
On: 07/28/23 10:37
The Brownshirts: Partie Deux; These aare the Muscle We've Been Waiting For
(3 total trackbacks)
Tracked at head to the Momarms site
The Brownshirts: Partie Deux; These aare the Muscle We’ve Been Waiting For
On: 03/14/23 11:20
Vietnam Homecoming
(1 total trackbacks)
Tracked at 广告专题配音 专业从事中文配音跟外文配音制造,北京名传天下配音公司
专业从事中文配音和外文配音制作,北京名传天下配音公司 北京名传天下专业配音公司成破于2006年12月,是专业从事中 中文配音 文配音跟外文配音的音频制造公司,幻想飞腾配音网领 配音制作 有海内外优良专业配音职员已达500多位,可供给一流的外语配音,长年服务于国内中心级各大媒体、各省市电台电视台,能满意不同客户的各种需要。电话:010-83265555 北京名传天下专业配音公司…
On: 03/20/21 07:00
meaningless marching orders for a thousand travellers ... strife ahead ..
(1 total trackbacks)
Tracked at Casual Blog
[...] RTS. IF ANYTHING ON THIS WEBSITE IS CONSTRUED AS BEING CONTRARY TO THE LAWS APPL [...]
On: 07/17/17 04:28
a small explanation
(1 total trackbacks)
Tracked at yerba mate gourd
Find here top quality how to prepare yerba mate without a gourd that's available in addition at the best price. Get it now!
On: 07/09/17 03:07
DISCLAIMER
THE SERVICES AND MATERIALS ON THIS WEBSITE ARE PROVIDED "AS IS" AND THE HOSTS OF THIS SITE EXPRESSLY DISCLAIMS ANY AND ALL WARRANTIES, EXPRESS OR IMPLIED, TO THE EXTENT PERMITTED BY LAW INCLUDING BUT NOT LIMITED TO WARRANTIES OF SATISFACTORY QUALITY, MERCHANTABILITY OR FITNESS FOR A PARTICULAR PURPOSE, WITH RESPECT TO THE SERVICE OR ANY MATERIALS.
Not that very many people ever read this far down, but this blog was the creation of Allan Kelly and his friend Vilmar. Vilmar moved on to his own blog some time ago, and Allan ran this place alone until his sudden and unexpected death partway through 2006. We all miss him. A lot. Even though he is gone this site will always still be more than a little bit his. We who are left to carry on the BMEWS tradition owe him a great debt of gratitude, and we hope to be able to pay that back by following his last advice to us all:
It's been a long strange trip without you Skipper, but thanks for pointing us in the right direction and giving us a swift kick in the behind to get us going. Keep lookin' down on us, will ya? Thanks.
- Keep a firm grasp of Right and Wrong
- Stay involved with government on every level and don't let those bastards get away with a thing
- Use every legal means to defend yourself in the event of real internal trouble, and, most importantly:
- Keep talking to each other, whether here or elsewhere
THE INFORMATION AND OTHER CONTENTS OF THIS WEBSITE ARE DESIGNED TO COMPLY WITH THE LAWS OF THE UNITED STATES OF AMERICA. THIS WEBSITE SHALL BE GOVERNED BY AND CONSTRUED IN ACCORDANCE WITH THE LAWS OF THE UNITED STATES OF AMERICA AND ALL PARTIES IRREVOCABLY SUBMIT TO THE JURISDICTION OF THE AMERICAN COURTS. IF ANYTHING ON THIS WEBSITE IS CONSTRUED AS BEING CONTRARY TO THE LAWS APPLICABLE IN ANY OTHER COUNTRY, THEN THIS WEBSITE IS NOT INTENDED TO BE ACCESSED BY PERSONS FROM THAT COUNTRY AND ANY PERSONS WHO ARE SUBJECT TO SUCH LAWS SHALL NOT BE ENTITLED TO USE OUR SERVICES UNLESS THEY CAN SATISFY US THAT SUCH USE WOULD BE LAWFUL.

Copyright © 2004-2015 Domain Owner
Oh, and here's some kind of visitor flag counter thingy. Hey, all the cool blogs have one, so I should too. The Visitors Online thingy up at the top doesn't count anything, but it looks neat. It had better, since I paid actual money for it.









